
Craniofacial Reconstruction Before & After Photos
Craniofacial Reconstruction Before & After 1
With a thin layer of skin and soft tissue over the brain, he was at high risk of trauma, infection, visual obstruction, and psychosocial harm.
Through the generous support and guidance of LEAP, Dr. Craig Hobar, and the Cheryl Lamon Memorial Fund, we were able to bring him to the United States and Medical City Dallas to perform the repair.
Dr. David Sacco performed the critical neurosurgical repair, removing nonfunctional brain tissue, and repairing the dura.
With Dr. Evan Beale, we used a pericranial flap, split calvarial bone grafts, orbital bone medialization, canthopexies, and skin tailoring, to provide further bone and soft tissue reconstruction.
He spent a few days in the hospital under close watch. He is seen at 7 weeks here, happy and thriving!

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.
Craniofacial Reconstruction Before & After 2
He came to us to correct his anterior open bite so that he could chew and speak more normally.
We were also able to improve his facial profile and balance, and he is breathing better now.
He is seen here at 6 weeks, with plans for further orbital and nasal reconstruction in the future.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.
Craniofacial Reconstruction Before & After 3
Previous efforts at another center to expand his skull and relieve the pressure with a shunt were unable to prevent blindness.
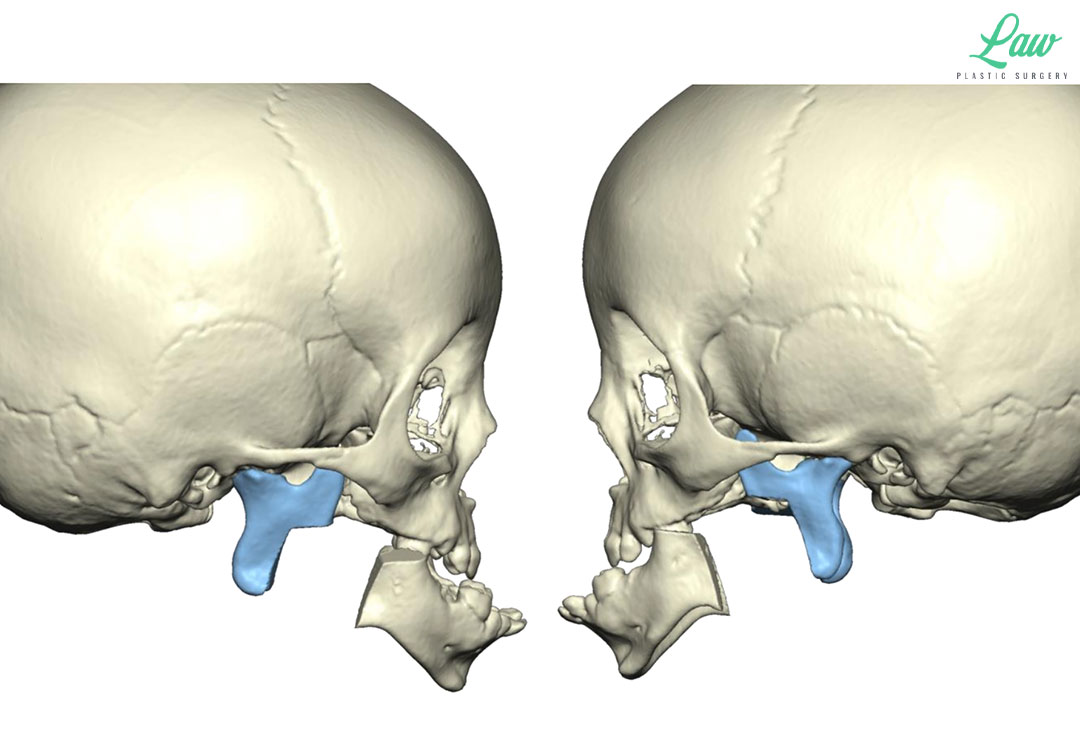
However, we did feel we could improve his midface hypoplasia (underdevelopment of the middle area of his face) with #distractionosteogenesis.
This was planned as a combined zygomatic repositioning and #LeFort II distraction.
In sequence, this was the same technique as a #LeFort III advancement and fixation, and then performing the LeFort II separation of the nasomaxillary segment with subsequent #externaldistraction to telescope the central area out even further.
While I usually prefer an internal distractor for a Lefort I, using the halo allowed for more control of the distraction in multiple planes, and for fixation against the cranium. #VirtualSurgicalPlanning helped guide us to the thickest bone on the cranium while avoiding the shunt in place.
He is seen here after removal of the distractor. Ideally we can now let him continue without any further surgery until skeletal maturity. At that point, I expect definitive #JawSurgery will be needed.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Craniofacial Reconstruction Before & After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.
Craniofacial Reconstruction Before & After 4
When the mandible is small and set too far back (microretrognathic),
–> the tongue falls back into the airway (glossoptosis),
–> and the airway is obstructed by the tongue.
The tongue can sometimes also be in the way of the palate as it closes, so a cleft palate may be present as well.
The treatment options include:
1) positioning on the baby’s stomach to let the tongue fall forward,
2) an oral airway plate to keep the tongue from falling back,
3) tongue-lip adhesion to pull the tongue forward,
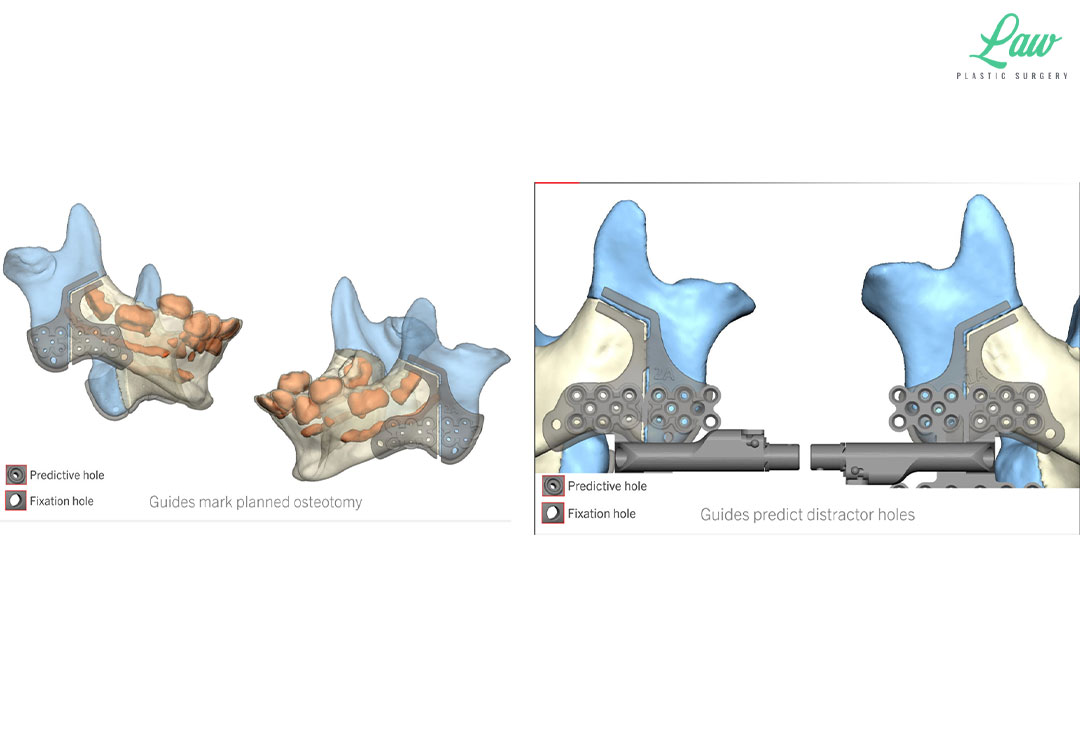
4) jaw distraction to carry the tongue forward as the mandible is pushed forward,
5) nasopharyngeal airway or tracheostomy to bypass the obstruction.
Here, distraction was done when other options had not done enough.
3D guides helped us to minimize risks to the tooth buds and inferior alveolar nerve.
After just a few days, he was able to be off of his home CPAP, and he has started catching back up with his growth and milestones.

Jaw Distraction Before and After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Jaw Distraction Before and After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.

Jaw Distraction Before and After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.
Jaw Distraction Before and After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.
Jaw Distraction Before and After Photo. Surgery performed in Dallas, TX at Law Plastic Surgery.